We carried out field research to understand how generic medicines are perceived by patients and pharmacists in everyday life:
- How is the topic discussed in pharmacies?
- What role does the pharmacist play in the choice between branded and generic medicines?
- How important is the quality of interaction with the patient?
The answers to these questions made it possible to understand the habits, needs and expectations of the actors in the health ecosystem. Attention was focused on the aspects that most influence the dynamics of the pharmacist-user relationship and sales and purchasing practices. In particular, the following were examined:
- the structure of the imagery of health and care that forms the background to patients’ interactions and concrete practices;
- the habits and attitudes of pharmacists and patients regarding off-patent and equivalent medicines, with the aim of measuring their level of activation and mapping the underlying value system;
- the analysis of the pharmacist’s experience and interaction with the patient.
Health and medicines
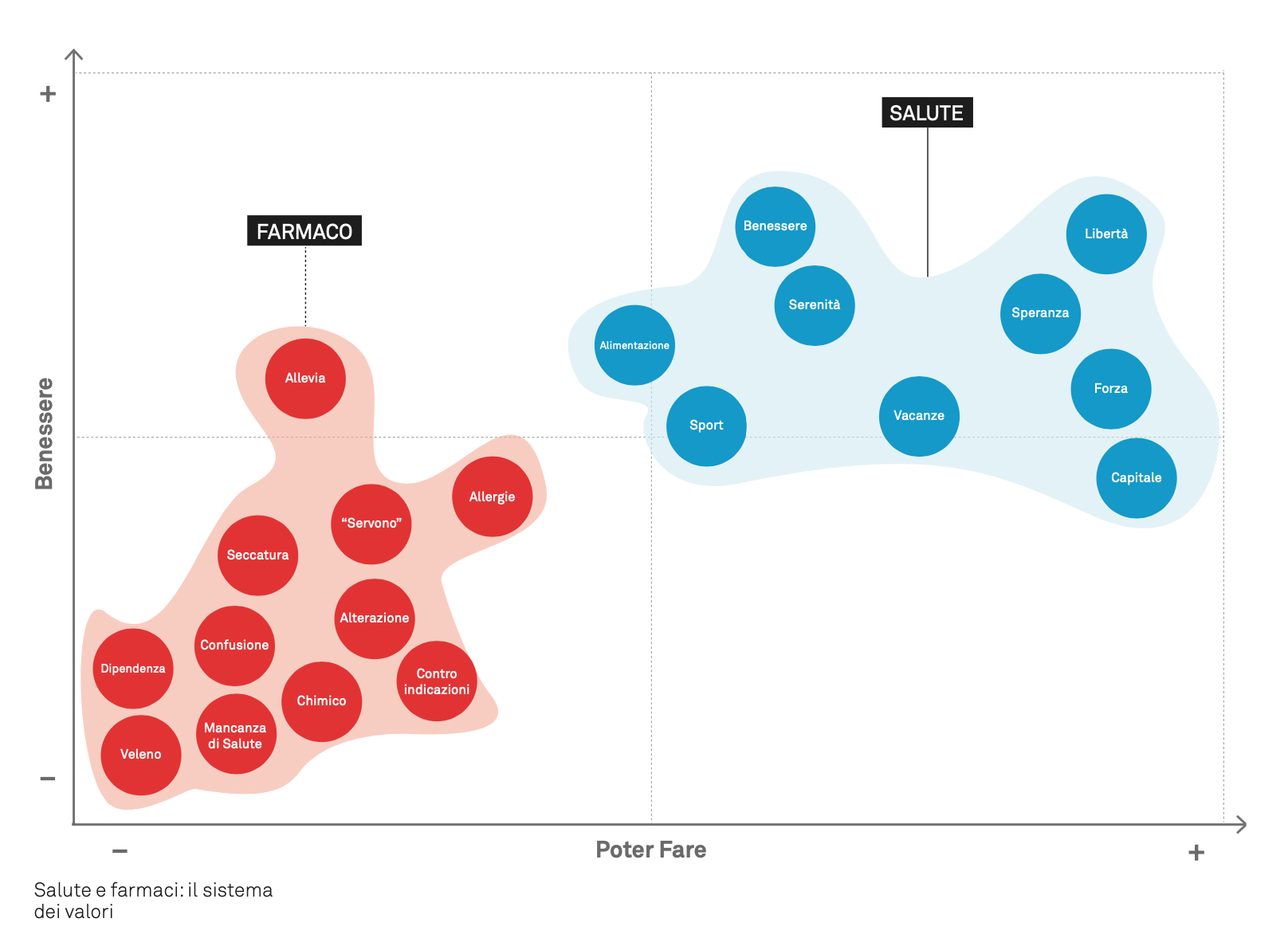
In patients’ imagery, health evokes a field of positive experiences and symbols. This positive connotation emerges from the narratives and definitions recorded during the focus group. Three recurring elements stand out:
- health is a condition of possibility, enabling people to act. Important values such as freedom and strength are associated with this element.
- Health is a basic existential condition. Important values and images such as hope, serenity and well-being are associated with this element.
- Connection with the body and its care.
Medicines, on the other hand, evoke a field of negative experiences and symbols, and only the “guarantee of healing” mitigates the negative perception of medicines. Among the many variations provided, three recurring elements stand out:
- medicines are experienced as an imposed, endured choice: one cannot do without taking them: «I need the antihistamine, I can’t not use it. If I don’t use it, what should I do?»;
- the very strong perception of the artificial nature («chemical») and harmful effects («poison», «contraindications») of medicines;
- the lack of adequate information and knowledge about medicines: «I don’t know what I’m taking», «if you read the leaflet, you get anxious», «even pharmacists are confused...».
Within the articulation of this imagery, the position of the theme of illness is particularly delicate. Patients tend not to make it explicit: illness disappears from the surface of discourse. Talking about one’s illness is embarrassing and complicated to share, because it makes people vulnerable and requires specific vocabulary. For these reasons, patients evoke it indirectly, by talking about medicines: the patients’ narrative focuses on the medicine, which takes on the weight of the topic and all its negative burden.
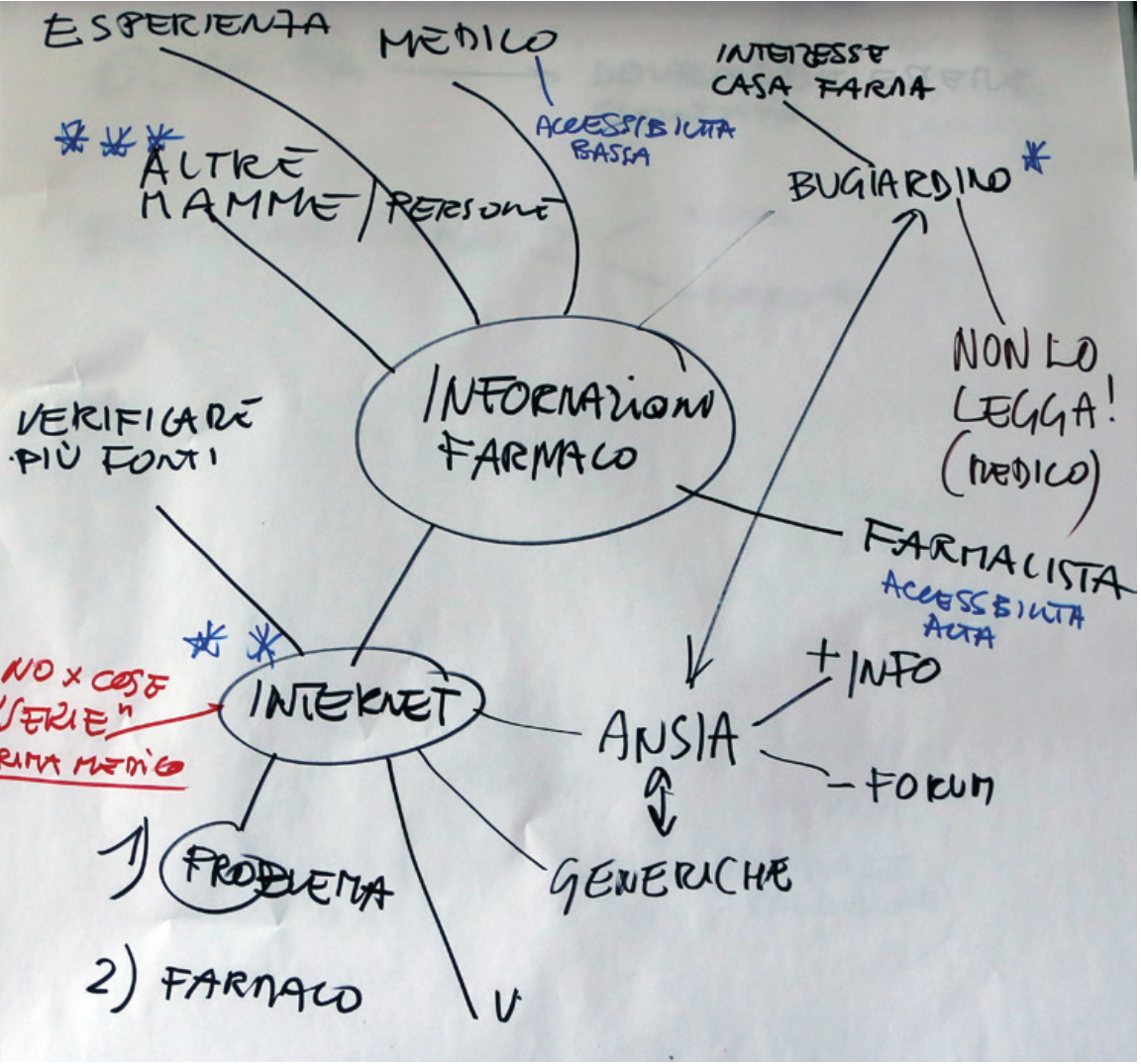
Information sources and awareness
Most patients build their knowledge of medicines and gather information about their health through a variety of channels and from very different sources in terms of type, legitimacy and authority. The importance of the source changes depending on the situations and issues on which the patient is called to make purchasing and care decisions. Differences in authority and legitimacy affect purchasing choices.
The first source is self-referential: experience, habit. Patients often need only confirmation from experience, or the gratification of having solved similar problems with the same medicine in the past. For mild conditions, or those perceived as such, a try & check approach is widespread:
The second is the close circle. Friends and relatives, colleagues or people who share characteristics and contexts similar to those of the patient:
Internet and social networks are sources that are always consulted, in some cases before any others. The Web is a reservoir of information about medicines, instructions for use, contraindications and side effects. Patients approach this wealth of information as they generally approach online content: with curiosity, to build background knowledge, but without attributing excessive credibility to it. The richness and heterogeneity of the information available generally escapes the control of patient-users. The result, not infrequently, is increased anxiety about one’s health status.
The doctor is the expert from whom patients expect certain and reliable advice on the most serious issues. Even though he or she is no longer necessarily at the top of the list of sources from which to obtain information about one’s health status.
Going to the doctor’s office is postponed over time, depending on the situation and the severity of the problems, but also on the possibility of finding information more simply and quickly from other sources. Overall, a certain marginality can be perceived, or rather a loss of centrality of the doctor’s figure within the patient’s imagery. Trust in the doctor is not in question. What emerges, rather, is a growing unwillingness to accept waiting times and the limited accessibility of one’s doctor’s office. Simply put, friends and relatives, the Web and the pharmacist are faster.
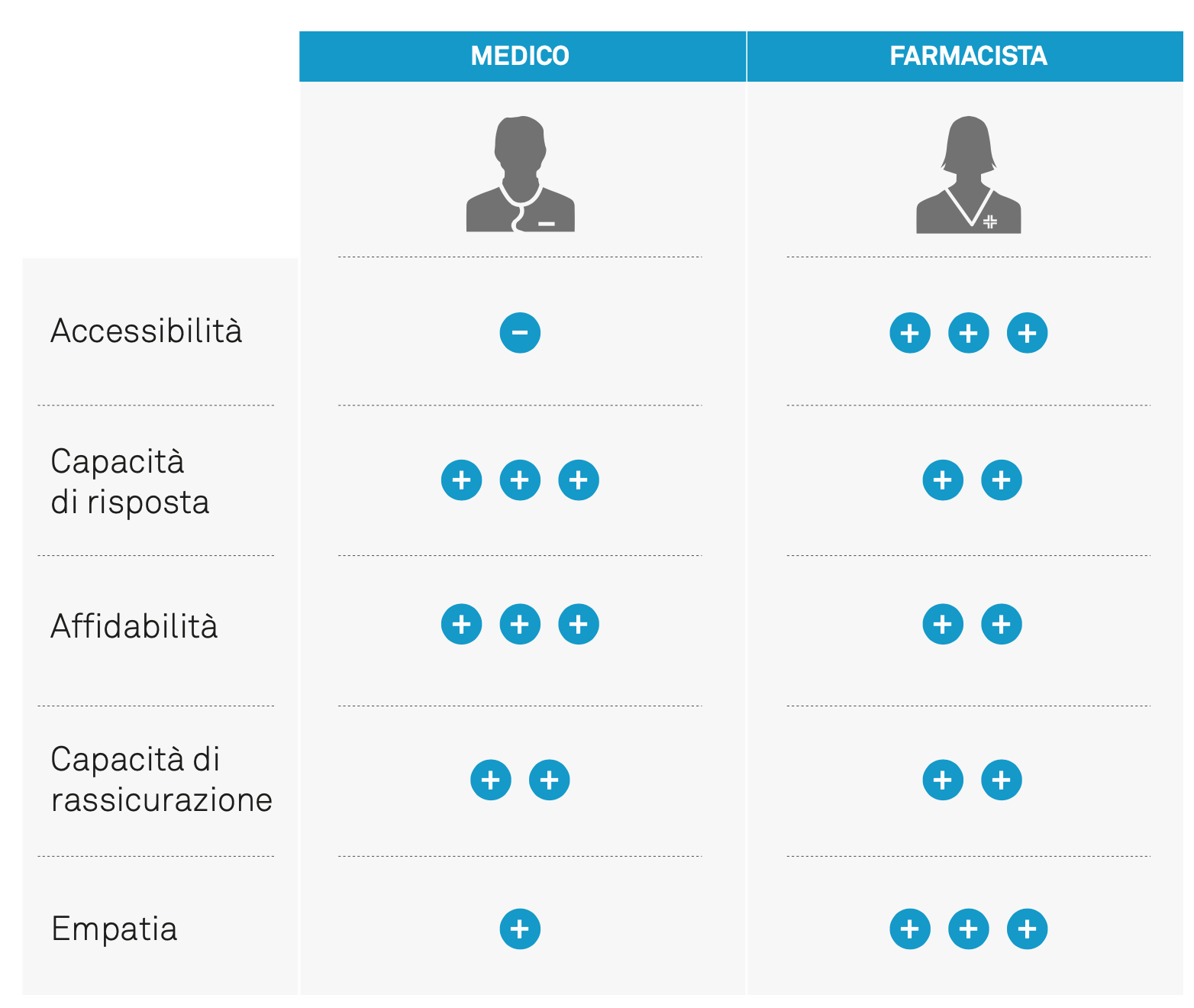
The presence of the pharmacist is the basis of the positive value attributed to the pharmacy. Patients tend to trust their pharmacist, recognizing an expertise that does not intimidate them. In patients’ perception, the pharmacist is the figure of balance and mediation between the system of medicines and that of health, represented by the limited availability of general practitioners and the bureaucratic hassles of hospitals and local health authorities.
If medicines evoke a negative imagery, in patients’ perception and judgment the pharmacy enjoys positive consideration. It is a safe space, where patients expect to find listening, guaranteed products and effective solutions. The credibility of the pharmacy as a space of value and safety reflects on everything that is sold, dispensed or provided there: body care products, personal hygiene products, and even food purchased in pharmacies are perceived as «better», «higher quality» than identical products available in supermarkets or parapharmacies.
Brand or generic
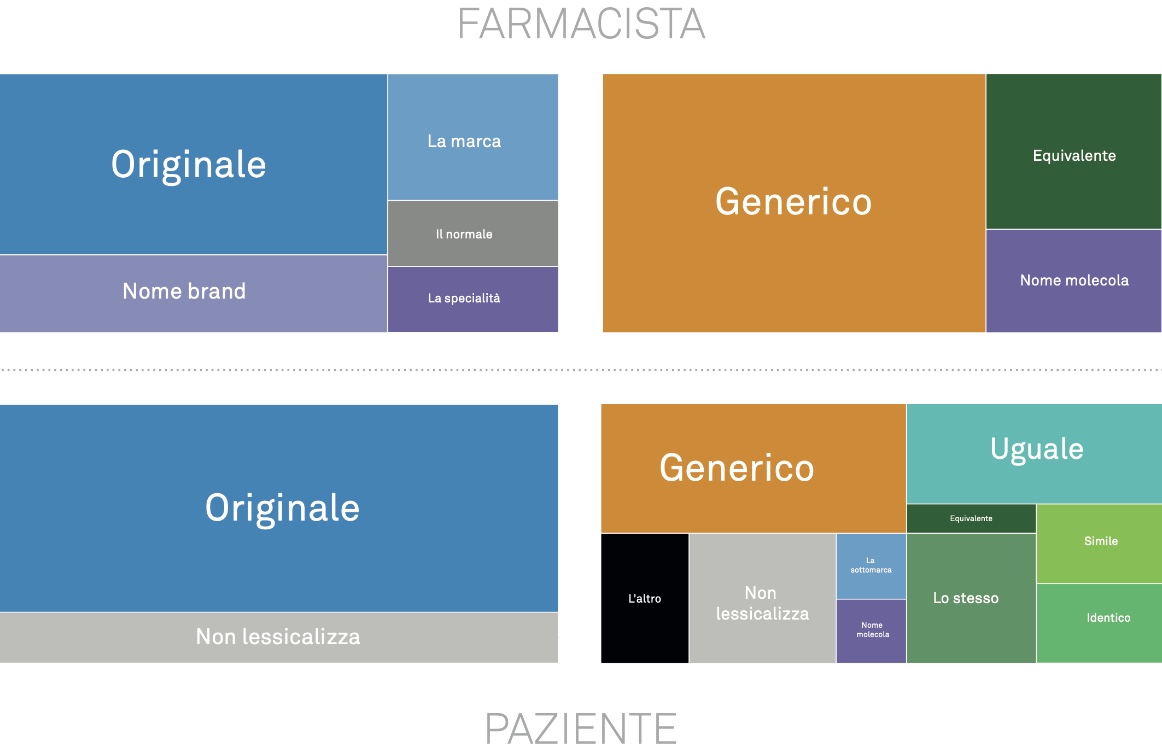
The introduction of the equivalent medicine has changed the semantics of the medicine and challenged patients’ linguistic skills. At the root of this competence is a certain way of representing the concept of medicine: in patients’ mental model, medicines are unique objects, identified by proper names and recognizable boxes: Tachipirina, Aspirina, Aulin, Tavor and Muscoril.
Difficulties arise the very moment the dual option must be represented. Pharmacists and doctors have found an answer by presenting the alternative between brand and equivalent in terms of original vs generic. It is in these terms that the alternative has become common sense: the brand is presented as the first choice, the cool product to prefer, while the generic is the second choice, the other one without quality, useful to save a little money if needed.
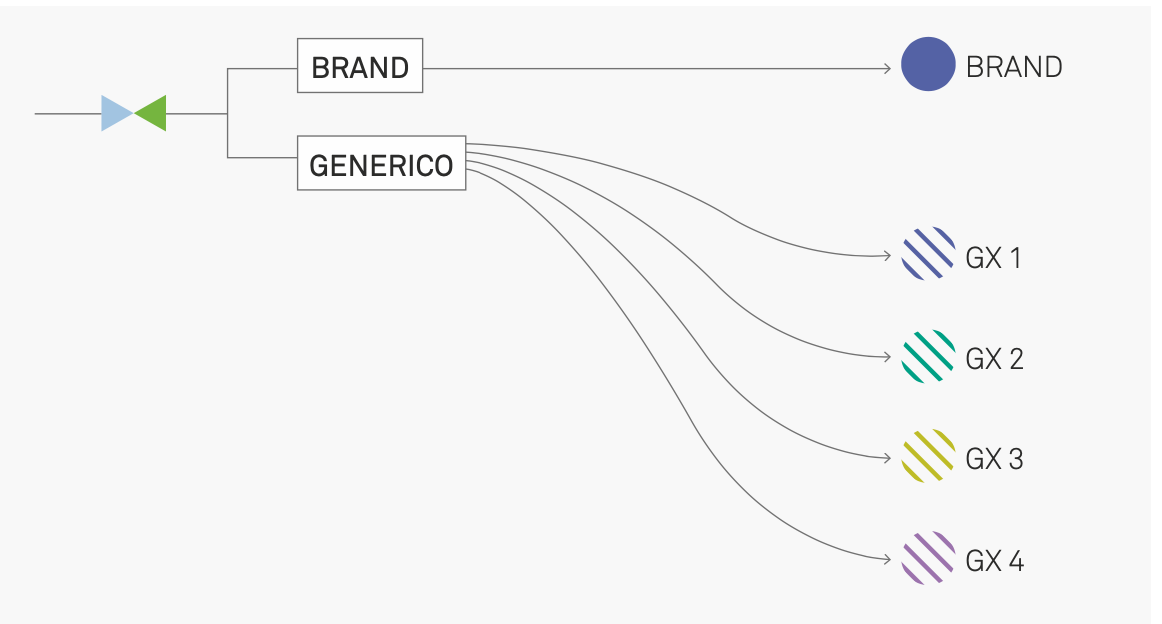
Another difficulty is added to these. The categories “branded medicine” and “equivalent medicine” are structured differently. The first is a structurally simple category – a set of unique objects identified by proper names (1:1 relationship between names and things). The second is more complex: the names of individual molecules are associated with n products from different brands: a set of weakly differentiated replicas (1:many relationship between names and things).
Equivalents, asymmetry and compliance
The multiplication of references and choice options puts compliance at risk. On this point, interviews with pharmacists reveal a common and widespread concern. Once the switch has been accepted, the patient is required to restructure their medicine-taking habits. Choosing the equivalent means dealing with a significant series of changes related to:
- the appearance of the packaging: changes in colors, name and size
- the shape
- the taste and color
This situation is complicated by the fact that, for the same equivalent, there are stylistic differences between the packaging of different generic companies. All these changes represent a strong constraint for patients, especially older ones, with consolidated therapeutic routines or therapies involving many medicines.

For this reason, pharmacists express concern and try to intervene. Many of the pharmacists interviewed have developed tools and practices to support patients and help them manage therapy correctly. At the same time, to limit the risk of error and disorientation, some decide to favor a single generic company.
Interaction in the pharmacy
In general, the pharmacy is at the center of a community of patients who visit it regularly, where people meet and recognize each other. The pharmacist is the custodian of the trust of the community members, whom they know and recognize in turn. Trust is built over time, through a mechanism of repeated confirmations.
At the basis of this relationship is a system of habits: purchasing habits, ways of presenting oneself in the store, recurring topics or visiting times, and so on. For some types of patients (older people, people with chronic conditions, mothers and parents of young children), this system is particularly consolidated. For them, purchasing in a pharmacy is a routine act, embedded within broader practices linked to caring for oneself and one’s loved ones, involving several actors in addition to the pharmacist (the family doctor, the specialist, the hospital...).
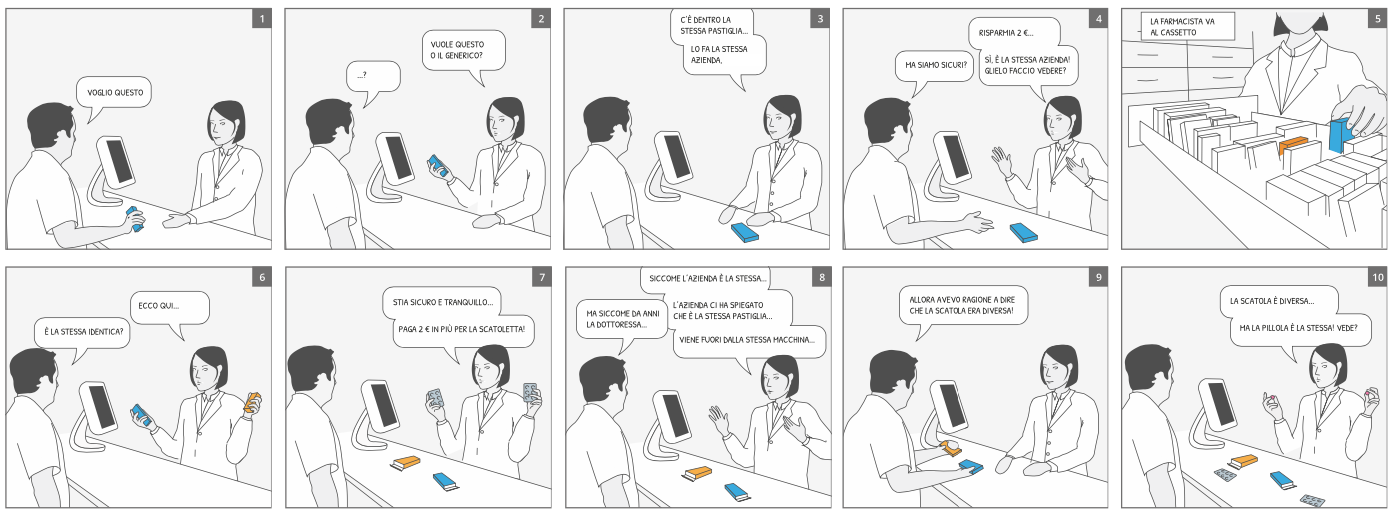
All interactions have precise phases and threshold moments that mark their end and the transition to the next one. In the face-to-face interaction between pharmacist and patient, the most important phase is the exchange, in which needs and offers are presented and local agreement on the solution is built: it may be automated and reduced to reading and responding to the prescription; it may be open, played out with style and, in any case, negotiated with a personal investment by the actors involved.
The priority of the interaction is the successful closure of the exchange; the quality of the relationship must be confirmed, regardless of the content of the exchange:
- the pharmacist wants to dispense the medicine and confirm their role as a trusted health expert;
- the patient wants to obtain the best solution and feel reassured by the visit to the pharmacy.
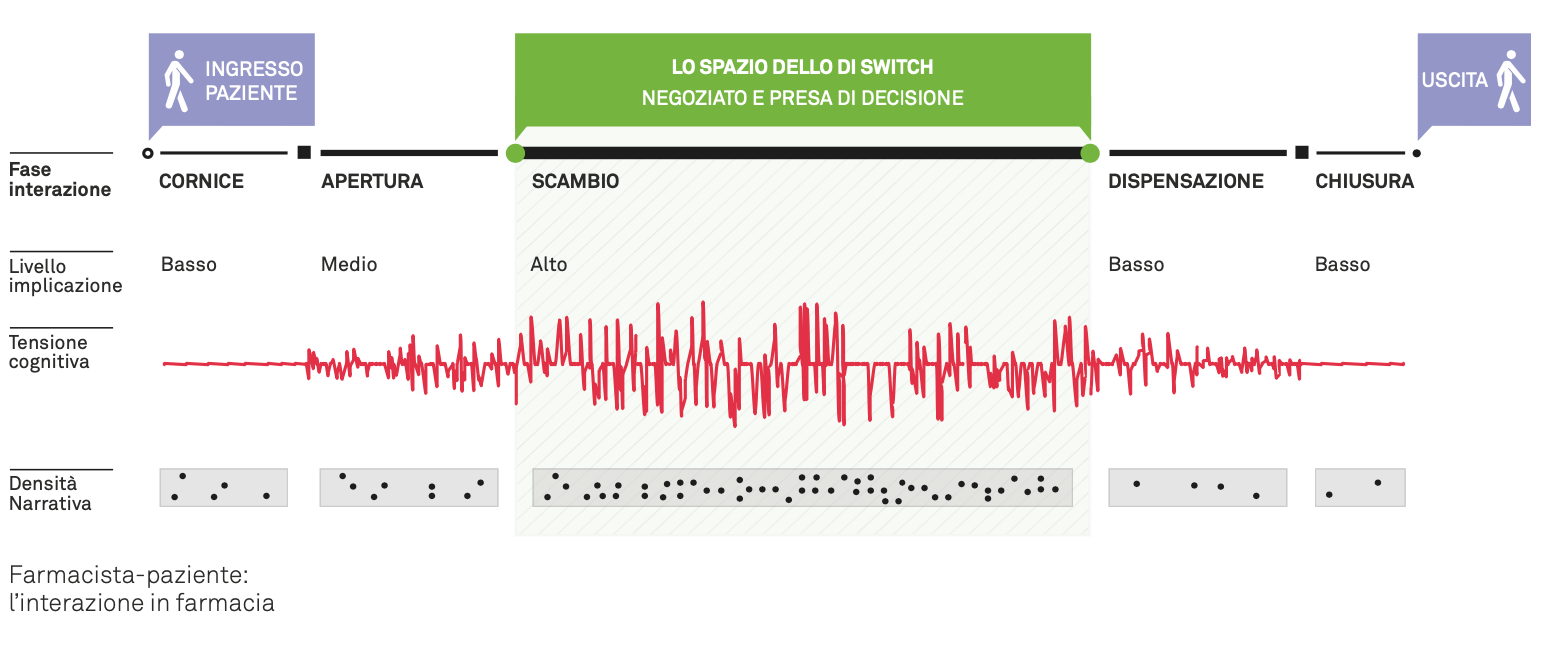
The proposal of the alternative between brand and equivalent is an integral part of this negotiation and represents its most delicate step, since the alternative, in most cases, is not transparent. The interaction becomes even more complicated if the patient asks the pharmacist for additional information or reassurance, or if they raise objections to the proposal of accepting the equivalent medicine instead of the corresponding brand. This work of explanation, reassurance and management of the many different objections has a decisive impact on the successful outcome of the ongoing interaction and is determined by numerous factors.
The analysis of the observed interactions revealed behavioral patterns and regularities. Three main factors influence the outcome of the switch:
- the type of prescription presented to the pharmacist;
- the patient’s profile in relation to the topic of the equivalent medicine (Convinced, Uncertain, Resistant);
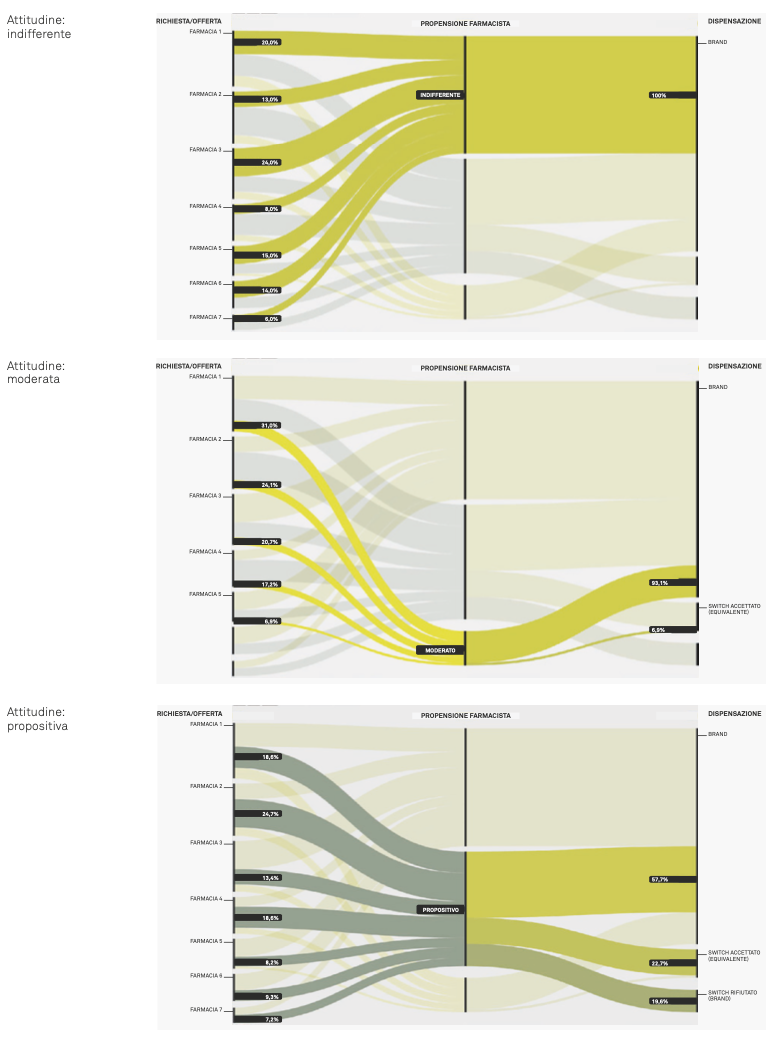
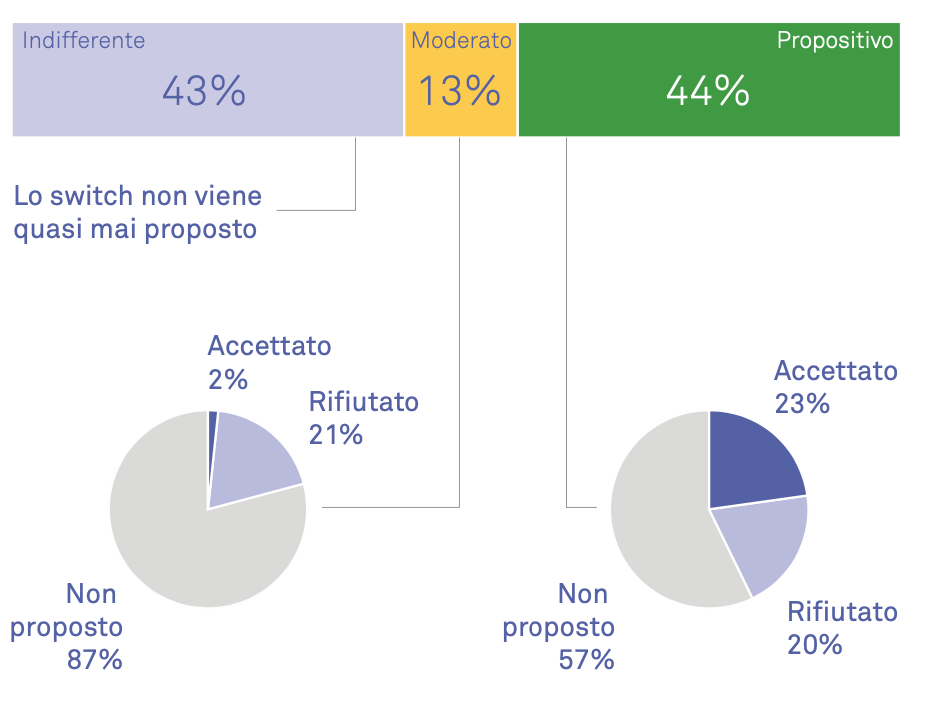
- the pharmacist’s attitude toward investing in the interaction and proposing the equivalent or not (Proactive, Moderate, Indifferent).
The switch
During the pharmacy observations, more than 300 pharmacist-patient interactions were observed. Attention focused on exchanges dedicated to the switch proposal and the management of the equivalent medicine topic.
It emerged that in about 70% of the recorded interactions, the pharmacist did not propose the switch; in the remaining 30%, however, the change was proposed. Within this 30%, three out of five times the patient accepted the substitution. In the remaining cases, they refused and purchased the brand. In the case of the indifferent pharmacist, the switch almost never takes place.